By Dr. Corrado Caporossi
Carious lesions appear most frequently in the pits and fissures of molars and premolars. The dental plaque inside pits and fissures cannot be removed through conventional cleaning techniques used in dental offices or through home care. The morphology of the fissure makes it difficult to diagnose the initial lesion, and surface decay may only become evident when the carious lesion has profoundly progressed beyond the amelodentinal limit.
In the past, clinicians used the “extension for prevention” approach to treat caries in pits and fissures. Thanks to new restorative techniques and bioactive materials, dentists can use minimally invasive approaches for more conservative cavity preparations, such as Preventive Resin Restorations (PRR). PRRs were first described by Simonsen and Stallard in 1977. Now PRRs can be performed with ionic composite resins, which restore the lesions in pits and fissures and help prevent recurrent caries in the rest of the fissure system.
Diagnosis of PRR
The clinical diagnosis for PRRs has three primary elements:
- Assessment of the patient’s caries risk
Document the patient’s medical history and perform testing as necessary to determine caries risk. - Diagnosis of lesion depth
Diagnose enamel lesions and not only cavitated lesions. This is important as the progression of the enamel lesion can be arrested. - Diagnosis of lesion activity
Both the activity of the lesion and the risk of caries are very important for diagnosis and treatment planning.
Indications for PRR
PRR can be performed on the occlusal surfaces of molars and premolars, buccal fossa of lower molars, and palatal sulcus of upper molars. They are indicated in both temporary and permanent dentition. A PRR is indicated when the carious lesion in the pits and fissures is small and discrete and confined only to the enamel, or when the process has reached the dentin, but without pulpal involvement.
Technique
The methods described above have evolved simultaneously with dental materials
and dentin adhesives. The PRR technique involves removing a minimal amount of
dental tissue with an air abrasion system with a 29-micron aluminum dioxide
powder. Caries removal may not reach the amelodentinal limit and may remain
confined to the superficial dentin. In both cases, selective etching should be
performed only on the enamel, followed by the application of a bonding agent.
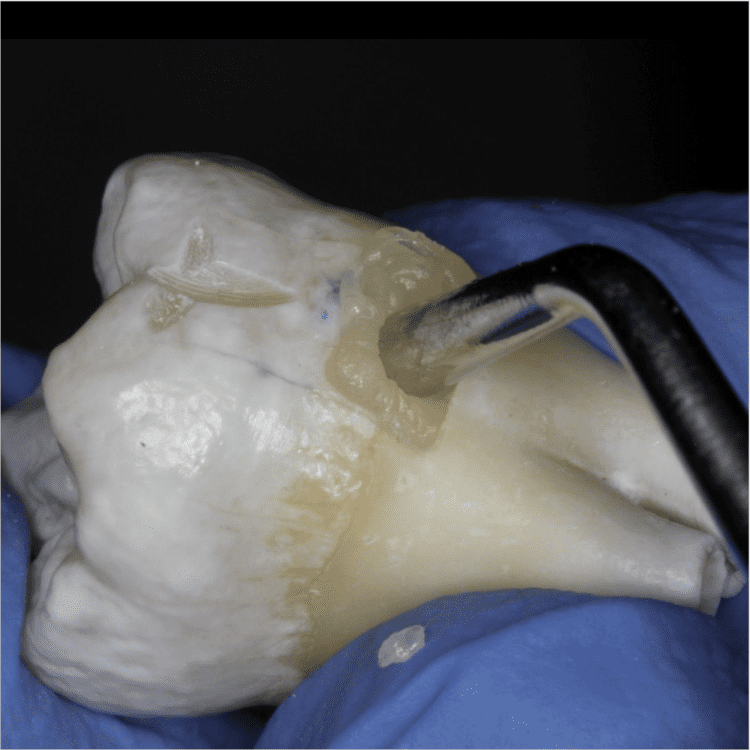
Subsequently, a dual-cure bioactive ionic resin (Activa Restorative Pulpdent) is applied and, after completing an initial 20-30 second self-curing phase, is covered with an oxygen inhibitor and light-cured. If the cavity is deeper, the clinician could use the sandwich technique, which consists of placing a fluid bioactive liner on the floor of the cavity (Activa Base/Liner Pulpdent) and then proceeding with the restorative material.
Case Study
A 15-year-old male patient presented with occlusal lesions on teeth #3.6 and #3.7 (#18 and 19) as shown in Figures 1 and 2. He was anesthetized and a rubber dam was placed. Anesthesia and absolute isolation with rubber dam are optional, depending on patient comfort and acceptance. The occlusal surface was cleaned with soft sandblasting, and caries was selectively removed with a small polymeric round bur in a conservative manner without cavity design (Figures 3 and 4). The cavo-surface angle was polished with an abrasive point to eliminate unsupported prisms. Areas of exposed dentin were covered with Teflon tape before selective etching enamel with a 37% orthophosphoric acid gel for 30 seconds. The surface was rinsed with water for 10-20 seconds and dried until it became chalky in color before applying a bonding agent. This was followed by placement of the bioactive resin (ACTIVA BioACTIVE-RESTORATIVE). For best results, allow the resin to self-cure for 20-30 seconds, cover with an air-block gel, and then light cure for 20 seconds on the low intensity setting. After removing the rubber dam, excess material was removed and the occlusion was checked.







About Dr. Corrado Caporossi
Dr. Corrado Caporossi received his degree in Dentistry and Dental Prosthetics at the European University of Madrid in Valencia, Spain where he completed a thesis on “Functional aesthetic rehabilitation in the anterior field with feldaspar ceramic veneers.” He is currently registered with the Order of Physicians and Dentists of Rome and is a member of AIO and ANDI. Dr. Caporossi is also an external professor at the Cardneal Herrera University of Valencia (Es.) and in the master courses of the University of Bari Aldo Moro. He carries out his professional activity in Labico (Rm) in his own dental microscopy center with a particular focus on partial aesthetic rehabilitions. Dr. Caparossi is a speaker at numerous national and international universities where he gives courses of advancement, and at national and international congresses where he discusses aesthetic reconstructive adhesive dentistry with the use of bioactive materials. He provides practical theoretical courses for training in and improvement of multidisciplinary restorative dentistry.
BIBLIOGRAPHY
Barrancos Mooney J. Tratamiento de lesiones incipientes: operatoria dental mínimamente invasiva. En Barrancos Mooney J, Barrancos P, eds. Operatoria dental.Integración clínica.4ª edición. Madrid: Editorial Médica-Panamericana; 2006.
Burke FJ. Restoration of the minimal carious lesion using composite resin. Dent Update 15 1988; 32: 234-232.
Crawford PJ . Sealant restorations (preventive resin restorations). An addition to the NHS armamentarium. Br Dent J 1988; 165:250-253.
Ekstrand KR, Ricketts DN, Kidd EA, Qvist V, SchouS. Detection, diagnosing, monitoring and logical treatment of occlusal caries in relation to lesion activity and severity: an in vivo examination with histological validation. Caries Res 1998;32: 247-54.
Llodra JC, Baca P, Bravo M. Selladores de fisuras. En: Bascones Martínez A. Tratado de Odontología. Tomo II. Madrid. Smithkline Beecham S A; 1998: 2249-57.
Nyvad B, Machiulskiene V, Baelum V. Reliability of a new caries diagnostic system differentiating between active and inactive caries lesions. Caries Res 1999; 33: 252-60.
Paterson RC, Watts A, Saunders WP, Pitts NB. Modern concepts in the diagnosis and treatment of fissure caries. Chicago: Quintessence Publishing Co; 1991.
Ripa LW, Wolff MS. Preventive resin restorations: indications, technique, and success. Quintessence Int 1992; 23:307-315.
Swift EJJ. Preventive resin restorations. J Am Dent Assoc 1987; 114:819-821.
BarrancosMoney J. Tratamiento de lesiones incipientes: operatoria dental mínimamente invasiva. En Barrancos Money J, Barrancos P, eds. Operatoria dental.Integración clínica.4ª edición. Madrid: Editorial Médica-Panamericana; 2006. PRÁCTICA 9 148 Burke FJ.
Restoration of the minimal carious lesion using composite resin. Dent Update 15 1988; 32: 234-232.
Crawford PJ . Sealant restorations (preventive resin restorations). An addition to the NHS armamentarium. Br Dent J 1988; 165:250-253.
Ekstrand KR, Ricketts DN, Kidd EA, Qvist V, SchouS. Detection, diagnosing, monitoring and logical treatment of occlusal caries in relation to lesion activity and severity: an in vivo examination with histological validation. Caries Res 1998;32: 247-54
Llodra JC, Baca P, Bravo M. Selladores de fisuras. En: Bascones Martínez A. Tratado de Odontología. Tomo II. Madrid. Smithkline Beecham S A; 1998: 2249-57
Nyvad B, Machiulskiene V, Baelum V. Reliability of a new caries diagnostic system differentiating between active and inactive caries lesions. Caries Res 1999; 33: 252-60
Paterson RC, Watts A, Saunders WP, Pitts NB. Modern concepts in the diagnosis and treatment of fissure caries. Chicago: Quintessence Publishing Co; 1991
Ripa LW, Wolff MS. Preventive resin restorations: indications, technique, and success. Quintessence Int 1992; 23:307-315. Swift EJJ. Simonsen RT, Stallard RE: Sealant restorations utilizing a diluted filled resin: one-year results. Quintessence Int 6:77-84, 1977.